Fetal anemia
Fetal anemia is a reduction in fetal hemoglobin concentration
Severity:
- Mild: Hb 0.8–1.0 MoM
- Moderate: Hb 0.55–0.8 MoM
- Severe: Hb <0.55 MoM
Clinical relevance starts once anemia is moderate or worse.
Etiologic classification
1. Immune fetal anemia
Caused by maternal IgG antibodies crossing placenta and destroying fetal RBCs.
Common causes:
- Rh(D) alloimmunization
- Other red cell antibodies:
- Kell (K)
- c, E
- Duffy, Kidd
2. Non-immune fetal anemia
A. Increased destruction
- Parvovirus B19
- Hemoglobinopathies
- Enzyme defects
- Microangiopathy
B. Decreased production
- Parvovirus B19 (pure red cell aplasia)
- Bone marrow failure syndromes
- Chromosomal disorders
C. Blood loss
- Fetomaternal hemorrhage
- Twin–twin transfusion
- Placental tumors (chorioangioma)
- Cord accidents
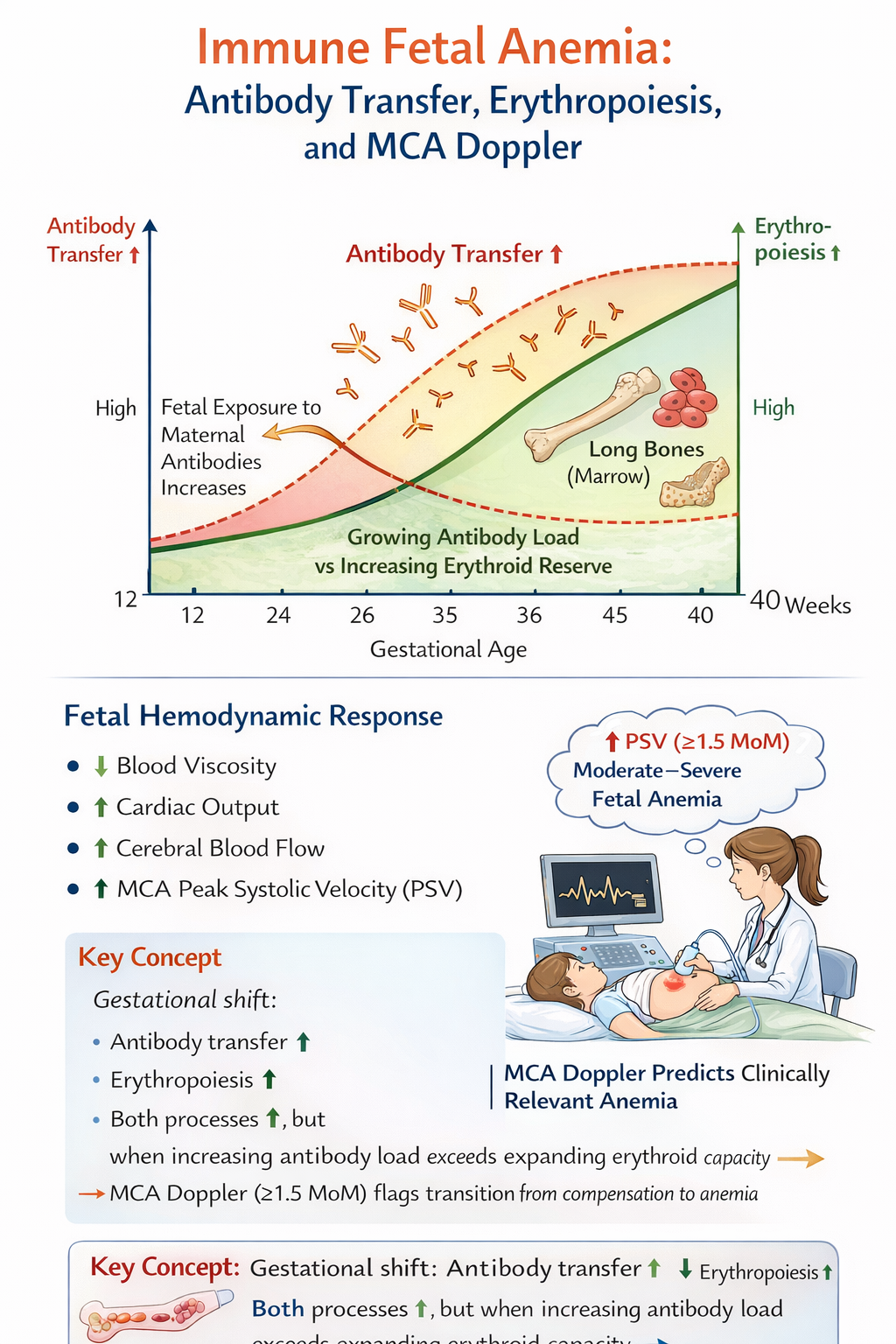
Pathophysiology
Anemia causes:
- ↓ blood viscosity
- ↑ cardiac output
- ↑ cerebral blood flow
Result:
- Increased peak systolic velocity in the MCA
Diagnosis of fetal anemia
1. Ultrasound signs (late, insensitive)
- Hydrops fetalis
- Ascites
- Skin edema
- Cardiomegaly
- Placental thickening
2. MCA-PSV Doppler (cornerstone)
Principle
- MCA-PSV correlates inversely with hemoglobin concentration.
Cutoff
- MCA-PSV ≥ 1.5 MoM → suggests moderate to severe anemia
Sensitivity and specificity
- Sensitivity for moderate–severe anemia: ~85–90%
- Specificity: ~75–80%
Very good for clinically actionable anemia.
Why mild anemia is often missed
This is critical and often underappreciated.
Reasons MCA-PSV misses mild anemia
- Hemodynamic compensation is subtle
- Blood viscosity change is minimal
- Physiologic overlap with normal fetuses
- Measurement variability
So: Mild anemia (Hb 0.8–1.0 MoM) can have normal MCA-PSV
Special situation: Kell alloimmunization
- Suppressed erythropoiesis
- Less hyperdynamic circulation
- MCA-PSV may underestimate severity
Management overview
Immune fetal anemia
Stepwise:
- Maternal antibody titers
- MCA-PSV surveillance
- Cordocentesis when indicated
- Intrauterine transfusion (IUT)
Non-immune fetal anemia
Treat cause when possible:
- Parvovirus → supportive ± IUT
- FMH → transfusion
- TTTS → laser therapy
Role of IVIG in immune fetal anemia
IVIG is used to:
- Reduce transplacental antibody-mediated hemolysis
- Delay onset or progression of fetal anemia
It does not replace IUT once anemia is established.
Indications for IVIG
Most commonly:
- Severe Rh or Kell alloimmunization
- History of:
- Early fetal demise
- Hydrops before viability
- High maternal antibody titers early in pregnancy
Used prophylactically, before anemia becomes severe.
Mechanism of action
IVIG:
- Saturates Fc receptors
- Reduces placental antibody transfer
- Modulates maternal immune response
Regimens (typical)
- 1 g/kg weekly, or
- 2 g/kg every 2–3 weeks
Started as early as 12–16 weeks in high-risk cases.
Effectiveness
- Delays need for first IUT
- Reduces severity of anemia
- Improves survival in severe alloimmunization
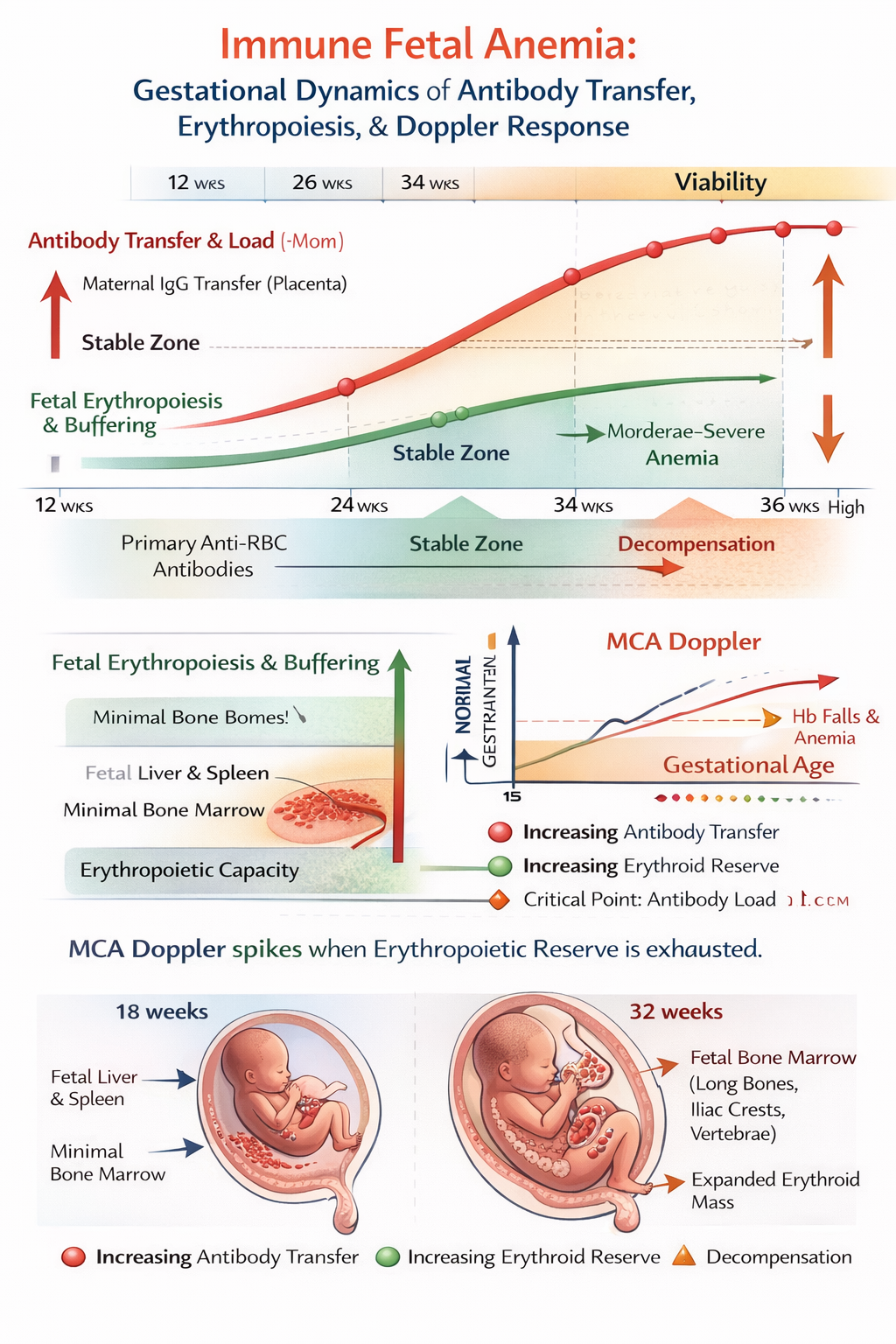
Age-dependent fetal adaptive response
1. Why fetal–maternal IgG transfer increases with gestation
Placental biology
- IgG transfer occurs via FcRn receptors on syncytiotrophoblast
- FcRn expression and placental surface area increase with
gestation
- Minimal transfer in early 2nd trimester
- Steep rise after 24–26 weeks
- Maximal transfer in 3rd trimester
Maternal antibody titers may be stable, but fetal exposure keeps rising.
This is why immune fetal anemia often worsens later, even without a rise in maternal titers.
2. The fetal counter-response: expanding erythroid reserve
The fetus responds on three levels: marrow expansion, extramedullary hematopoiesis, and physiologic adaptation.
3. Erythropoiesis shifts with gestational age
Early gestation
- Liver and spleen dominate erythropoiesis
- Bone marrow contribution is limited
- Low reserve, poor buffering capacity
- Early immune anemia progresses rapidly
- Hydrops can occur with modest antibody exposure
Mid to late gestation: marrow takes over
By ~20–24 weeks:
- Bone marrow becomes the primary erythropoietic organ
- Progressive recruitment of:
- Long bones
- Iliac crest
- Vertebrae
- Ribs
By the third trimester:
- Iliac crest and long bones are major RBC factories
- Total erythroid mass and turnover capacity increase sharply
4. Expansion of the erythroid base (the key concept)
With rising maternal IgG transfer, the fetus compensates by:
1. Increasing erythropoietin (EPO)
- Produced mainly by fetal liver and kidneys
- Rises exponentially in anemia
- Drives marrow hyperplasia
2. Marrow recruitment and expansion
- Long bones and iliac crests show:
- Increased erythroid precursors
- Increased reticulocyte output
- This buffers antibody-mediated hemolysis
Clinically:
- Same antibody titer causes less severe anemia later than earlier
3. Extramedullary hematopoiesis
- Liver and spleen re-expand production
- Leads to:
- Hepatosplenomegaly
- Increased cardiac preload
This is compensatory, not pathologic initially.
5. Fetal "behavioral" and physiologic responses to anemia
As anemia increases, the fetus shows predictable responses:
Hemodynamic
- ↑ cardiac output
- ↓ blood viscosity
- ↑ cerebral perfusion (MCA-PSV rise)
Movement and tone
- Early anemia: normal movements
- Moderate anemia: increased activity (hyperdynamic state)
- Severe anemia: ↓ movements (pre-terminal)
6. Fetal anemia may appear "stable" despite rising antibody titers
- Maternal antibody transfer ↑
- Antibody titers stable or rising
- Yet:
- MCA-PSV remains <1.5 MoM
- Hydrops absent
The expanding erythroid base and increasing marrow productivity temporarily outpace hemolysis.
This buffering capacity:
- Improves with gestation
- Is much better after 26–28 weeks
- Is why late disease can look deceptively mild
7. Why this compensation eventually fails
Compensation fails when:
- Hemolysis exceeds production
- Or marrow function is impaired
Examples:
- Kell alloimmunization
- Antibodies suppress erythroid progenitors
- Erythroid base cannot expand effectively
- Doppler underestimates severity
- Very high antibody load
- Superimposed infection or hypoxia
8. Clinical implications
1. Timing matters more than titer
- Same titer at 18 weeks ≠ same risk at 32 weeks
- Early disease is more dangerous
2. MCA-PSV reflects physiology, not antibody burden
- Stable Dopplers mean compensation is holding
- Sudden rise means reserve is exhausted
As gestation advances:
- Antibody exposure ↑
- Placental transfer ↑
- Erythroid capacity ↑ even more
Disease severity depends on which curve rises faster.
A. Maternal–fetal IgG transfer
- IgG transfer across the placenta is minimal before 16–18 weeks
- It rises steeply after 24 weeks
- Peaks in the third trimester, often exceeding maternal levels
So paradoxically, the fetus is exposed to more antibody later, not earlier.
B. Fetal erythropoietic capacity increases with gestation
Early gestation:
- Limited erythropoiesis
- Liver-dominant, small marrow volume
- Minimal reserve
Later gestation:
- Expansion of erythroid niches:
- Bone marrow (long bones, ribs, vertebrae)
- Iliac crest
- Increased erythropoietin responsiveness
- Faster reticulocyte release
- Ability to mount compensatory erythropoiesis
This is why many fetuses tolerate rising antibody titers for a long time before decompensating.
3. Hemodynamic response to anemia is age-independent
When fetal anemia develops, regardless of gestational age, the fetus shows a stereotyped cardiovascular response:
- Reduced blood oxygen content
- Cerebral vasodilation
- Reduced blood viscosity
- Increased cardiac output
- Increased systolic velocity in cerebral arteries
These responses are qualitatively the same at 18 weeks and at 32 weeks.
Clinical implications
- Rising maternal antibody titers alone do not mandate intervention
- Surveillance should focus on:
- MCA-PSV trends
- Not absolute gestational age
- IVIG delays anemia by reducing hemolysis, effectively buying time for erythroid compensation
- MCA Doppler detects the point at which compensation fails