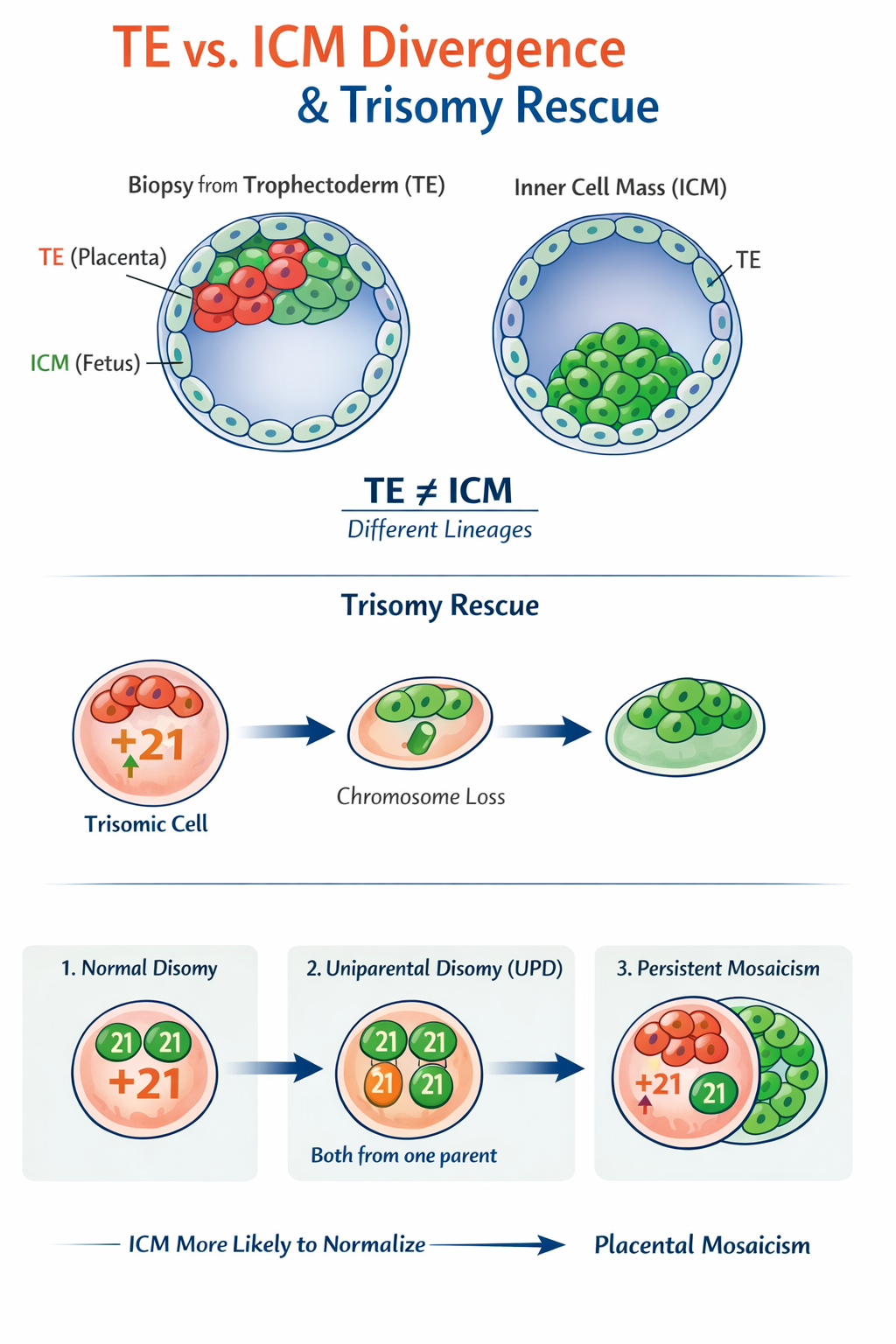
PGT-A samples trophectoderm (TE) cells, not the inner cell mass (ICM).
- TE
- Forms placenta and membranes
- Higher tolerance for aneuploidy
- Actively proliferating, genomically unstable early on
- ICM
- Forms the fetus
- Under stronger selection pressure
- More likely to normalize via selection and apoptosis
So PGT-A is placental genetics at blastocyst stage, not fetal genetics.
This explains:
- Mosaic calls
- Chaotic calls
- False positives
- Normal babies after “abnormal” PGT-A
Origins of mosaicism
Most mosaicism detected on PGT-A is post-zygotic mitotic error, not meiotic nondisjunction.
- Anaphase lag
- Mitotic nondisjunction
- Chromosome mis-segregation during rapid cleavage
This creates lineage-restricted mosaicism:
- Abnormal cells preferentially populate TE
- Normal cells preferentially populate ICM
This is NOT theoretical & WELL documented in:
- CVS vs amniocentesis discordance
- Placental confined mosaicism (CPM)
Interpreting PGT-A result categories
1. Euploid
- All tested TE cells appear balanced
- Still not “guaranteed normal”
- Resolution limits apply (segmental <5–10 Mb may be missed)
Implantation potential: Highest
2. Aneuploid (uniform)
- Same whole chromosome gain/loss across sampled TE cells
- Often meiotic in origin
- But even here:
- TE ≠ ICM
- Trisomy rescue is possible (more below)
Implantation potential: Low but not zero
3. Mosaic
Typically reported as 20–80% abnormal signal.
What mosaic really means:
- Mixed cell population in the biopsy
- Or technical noise amplified by WGA
- Or true confined placental mosaicism
Important nuance:
- Low-level mosaic (20–40%)
- Often TE-limited
- High chance of normal ICM
- High-level mosaic (40–80%)
- More likely true embryo-wide involvement
- Still not deterministic
Implantation potential:
- Lower than euploid
- Much higher than uniform aneuploid
- Chromosome-specific effects matter (16, 22 worse than 15, 21)
4. Chaotic / complex aneuploidy
- Multiple whole chromosomes and segments gained/lost
This is the most misunderstood category.
What “chaotic” usually reflects:
- Early cleavage-stage genomic instability
- Mitotic catastrophe in TE lineage
- WGA amplification artifacts exaggerating noise
Crucial insight:
Chaotic TE does not necessarily mean chaotic ICM
True genetic makeup of the fetus
Amniocentesis beats PGT-A
- Amniocytes derive from epiblast
- They reflect fetal lineage
- This is why:
- CVS can be abnormal
- Amnio can be normal
- Baby can be normal
Trisomy rescue: the great normalizer
What is trisomy rescue
Loss of one chromosome from a trisomic cell to restore disomy.
Occurs:
- Early post-implantation
- More commonly in ICM than TE
Outcomes:
- Normal disomy
- Uniparental disomy (UPD)
- Persistent mosaicism
This explains:
- Normal fetuses after trisomic embryos
- Placental mosaicism with normal baby
- UPD syndromes after “self-correction”
| Chromosome | Rescue likelihood | Clinical implication |
|---|---|---|
| 16 | High | Common CPM, often normal fetus |
| 22 | Moderate | Risk of growth issues |
| 15 | Moderate | UPD risk (Prader–Willi / Angelman) |
| 21 | Low | Persistent trisomy more likely |
| 13, 18 | Low | Poor developmental tolerance |
This is why trisomy 16 mosaic embryos sometimes do surprisingly well.
Implantation potential:
Determinants stronger than PGT-A label
- Endometrial receptivity
- Embryo metabolic competence
- Mitochondrial health
- Synchrony between embryo and uterus
PGT-A mostly predicts:
- Likelihood of implantation
- Not certainty of fetal outcome
Rate-limiting step is attachment and heartbeat
Once implantation succeeds and heartbeat establishes, selection has already happened.
Why PGT-A overcalls abnormality
Technical contributors
- Whole genome amplification bias
- Low DNA input
- GC-content variability
- Bioinformatic smoothing thresholds
A 5-cell TE biopsy represents:
- <1% of the embryo
- From a lineage not destined to become fetus
False positives are EXPECTED.
Key
“PGT-A tells us about implantation potential, not the final genetic makeup of the
baby.”
Invasive prenatal testing still matters
- Even after euploid PGT-A:
- De novo CNVs
- Segmental imbalances
- Mosaicism resolution
Amniotic CMA remains the gold standard for fetal genetics.